Background:
Selecting an antipsychotic medication can be a difficult process and there are not many trials that compare the medications to each other. Breaking down the selection into a few steps can simplify the process.
- First, I look for the indication. What are you using the antipsychotic for? Even though these medications are called “antipsychotics,” they are used for many reasons. Some examples include depression, bipolar mania, bipolar depression, schizophrenia, irritability associated with autism, and Tourette’s disorder. Knowing the indication is very important because some medications are only effective for some indications. For example, aripiprazole is approved as an adjunct for depression, but haloperidol is not.
- Next, I look for history. If a family member of the patient has successfully been treated with a medication, then the patient themselves are more likely to also respond to that medication. I also need to know what medications the patient has tried in the past. If something worked, I may select that medication again or something similar, or if something caused side effects, then I will pick something very different.
- Finally, I look at side effects. Although these medications can be helpful they can also cause a lot of side effects. Knowing the side effects can be extremely helpful in medication selection. For example, I will avoid something like olanzapine if a patient wants to avoid weight gain.
Schizophrenia:
There are guidelines from around the world that recommend how to treat schizophrenia. I included guidelines for the United States, Canada, and the United Kingdom.1,2,3,4 The guidelines are broad and do not recommend a specific treatment other than clozapine for treatment resistant schizophrenia.

A famous study called the CATIE trial compared some of the antipsychotics in 1,400 patients. They followed the patients for 18 months. A general conclusion of the trial was that the antipsychotics seem to be as effective as each other, so the choice of the agent should be based on side effects.5
Bipolar disorder:
Bipolar disorder is generally broken down into mania, or depression. It can get more complicated with “mixed states” and other disease states but we will focus on bipolar mania and bipolar depression. Although there are specific medications that are approved for bipolar mania, most antipsychotics will treat mania. Bipolar depression is trickier. Some antipsychotics have evidence that they work, but others like aripiprazole, have evidence that they don’t work for bipolar depression.6,7

Major depressive disorder:
Antipsychotic medications are sometimes used in major depressive disorder (MDD). Most of the time, the antipsychotic is added to an antidepressant. There is a small amount of data for using an antipsychotic like quetiapine alone in depression.8 Antipsychotics are most helpful in a type of depression called “depression with psychotic features.” Sometimes when people become depressed, they start hearing things or seeing things that others don’t see. This is different from schizophrenia because in MDD with psychotic features, the psychosis is only present when the person is depressed.
Delirium and dementia:
Delirium is a sudden confusion while dementia is long term cognitive decline. Someone with dementia can also become delirious. Sometimes antipsychotics are used in both delirium and severe behaviors associated with dementia.

Antipsychotics are reserved for very serious behavioral complications in someone with dementia. For example if someone is being violent, assaultive, or sexually inappropriate. The reason antipsychotics are reserved in dementia is because there is an increased mortality risk in elderly patients. There is a black box warning based on a meta analysis that showed 15/17 trials (9 unpublished) had an increased risk of death in older adults (3.5% vs 2.3%).9
Acute agitation or aggression:
Antipsychotics are also often used in the emergency room to calm down a patient who is aggressive or violent. Sometimes patients are under the influence of substances or agitated and the short term use of an antipsychotic, along with sedatives are commonly used.
Safety and side effects:
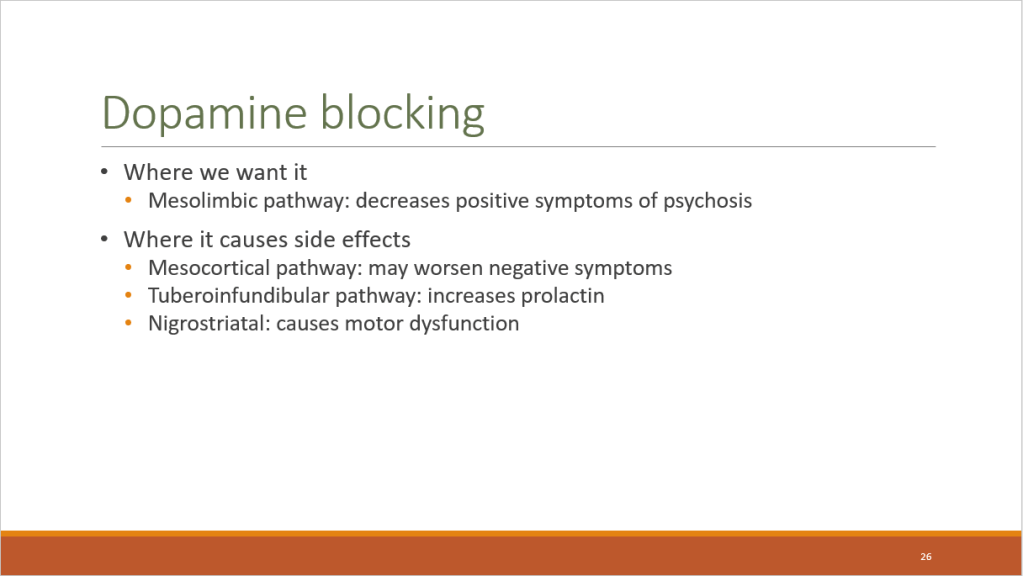
The first set of side effects are from blocking a receptor in the brain for a neurotransmitter called dopamine. We are able to target specific receptors, but we aren’t good at targeting a specific pathway or area of the brain.
Metabolic side effects are seen below:

Anticholinergic effects are seen below:

Other side effects can be very serious. One is that antipsychotics can lower the seizure threshold. This means that seizures are slightly more likely to occur and can even occur in those without a seizure history. Clozapine (dose related) and chlorpromazine are some of the biggest offenders.
Antipsychotics can also prolong a measurement on an electrocardiogram called a QTc. If used in combination with other QTc prolongers, serious arrhythmias can occur. Some of the biggest offenders are ziprasidone, thioridazine and pimozide. Lurasidone is an antipsychotic without a QTc warning.
Finally, antipsychotics can cause a life-threatening condition called Neuroleptic malignant syndrome. This is characterized by rigidity, autonomic instability, and cognition changes. Treatment is immediately required.
Conclusion:
Selecting an antipsychotic can be difficult, but breaking down the selection into a few steps can be helpful.

References:
- Hasan A, Falkai P, Wobrock T, Lieberman J, Glenthoj B, Gattaz WF, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of schizophrenia, part 1: update on the acute treatment of schizophrenia and management of treatment resistance. World J Biol Psychiatry. 2012;13(5):318-78.
- National Institute for Health and Care Excellence. Psychosis and schizophrenia in adults: prevention and management. Available at nice.org.uk/guidance/cg178.
- Remington G, Addington D, Honer W, Ismail Z, Raedler T, Teehan M. Guidelines for the pharmacotherapy of schizophrenia in adults. Can J Psychiatry. 2017;62(9):604-16
- Keepers G, Fochtmann L, Anzia J, et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Schizophrenia. Third Edition. Dec 2019.
- Liebermann J, Stroup T, McEvoy J, et al. Effectiveness of Antipsychotic Drugs in Patients with Chronic Schizophrenia. N Engl J Med 2005;353:1209-23.
- Thase M, Jonas A, Khan A, et al. Aripiprazole monotherapy in nonpsychotic bipolar I depression: results of 2 randomized, placebo-controlled studies. J Clin Psychopharmacol. 2008 Feb;28(1):13-20.
- Yatham L. A clinical review of aripiprazole in bipolar depression and maintenance therapy of bipolar disorder. J Affect Disord. 2011 Jan;128 Suppl 1:S21-8.
- Weisler R, Montgomery S, Earley W, et al. Efficacy of extended release quetiapine fumarate monotherapy in patients with major depressive disorder: a pooled analysis of two 6-week, double-blind, placebo-controlled studies. Int Clin Psychopharmacol. 2012 Jan;27(1):27-39.
- Schneider L, Dagerman K, Insel P. Risk of Death With Atypical Antipsychotic Drug Treatment for Dementia Meta-analysis of Randomized Placebo-Controlled Trials. JAMA. 2005;294(15):1934-1943.
